Updated: August 19, 2022
Pelvic congestion syndrome, also called pelvic venous congestion, falls under a broader range of pelvic venous disorders which are a known, but often unrecognized cause of chronic pelvic pain. Varicose pelvic veins develop when the valves in veins are not working correctly, or occasionally when critical deeper veins are obstructed, causing blood to pool and distend pelvic veins.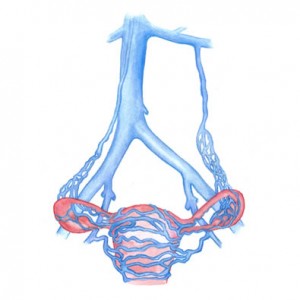
To explain pelvic congestion syndrome, it it helps to understand the purpose of veins in the body:
Healthy veins return blood to the heart through one-way valves, allowing blood to travel toward the heart. Congested veins have weakened valves, allowing blood to flow backward and pool distend and pelvic veins.
Occasionally, increased pressure inside pelvic veins may be the result of an obstruction in the major veins draining the pelvis.
Commonly Recognized Associations
It is estimated that 30% of patients with chronic pelvic pain of an unknown cause actually suffer from a symptomatic pelvic venous disorder. Although the causes of pelvic venous congestion are complex and poorly understood, a few commonly recognized associations include:
- Family history of venous disease
- Multiple pregnancies
- Estrogen
- Pelvic or renal vein compression
What Are the Symptoms of Pelvic Congestion Syndrome?
Typical symptoms of pelvic congestion include:
- Increased urination frequency
- Bloating sensation
- Visible varicose veins on the buttocks, vulva, and upper thighs
- Dull achiness and/or heaviness in the pelvis, often made worse by prolonged standing
- Painful menstrual cycles with referred pain in the legs
- Pain during and after intercourse
How Is Pelvic Venous Congestion Diagnosed?
Unfortunately, pelvic venous congestion often goes unrecognized and untreated. Symptoms, physical exam and ultrasound findings have a high combined predictive value in diagnosing pelvic venous disorders. The ability of duplex ultrasound (DUS) to image real-time makes it an important tool in the evaluation of possible pelvic venous congestion.
Because there are many other potential causes of chronic pelvic pain, medical professionals may conduct multiple exams and tests including:
- Pelvic exam
- Pelvic duplex ultrasound
- CT or MRI scan
- Laparoscopy
In our office, a nurse practitioner, physician’s assistant, or physician will discuss pelvic symptoms with you. They will determine whether you present with pelvic congestion syndrome symptoms and order an ultrasound to look for varicose veins in the pelvis, labial area, and upper thigh. This gives information regarding the sizes of the varicose veins in the pelvis and whether they have propagated to other parts of the body. Once these veins are found, they will also order a CT scan to show the origin of the varicose veins.
Treatment
Once a patient is diagnosed with pelvic venous congestion, it can often be successfully treated with a minimally invasive procedure called embolization. Pelvic venous embolization requires little or no downtime and is performed in an outpatient setting. Occasionally, a compressed iliac vein may contribute to venous congestion and a stent may be indicated to help restore normal flow.
Benefits of embolization:
- Requires little or no downtime
- Performed as an outpatient
- Minimally invasive, but highly effective
After treatment, patients are typically able to return to most routine activities the same day.
Ovarian Vein Embolization Treatment Tips
- Wear comfortable clothing to the procedure
- Eat a light meal the evening before your procedure
- Don’t eat or drink less than 6 hours before treatment, unless directed by your doctor
- Over-the-counter pain medication is typically all that is needed after the procedure
- While recovering, stay active but avoid heavy lifting
- Reach out to your treating doctor with any questions or concerns
Follow Up
We always follow-up with the patient approximately one month post venogram to see if some you the patient’s symptoms have resolved. It may take 1-2 menstrual cycles before significant relief is noticed. Most women we have seen in the office for their post venogram follow-up have described some cramping for the first few days post procedure, and with significant relief in the weeks and months after.
For more information on pelvic congestion syndrome visit: Pelvic Congestion Syndrome

